Blog
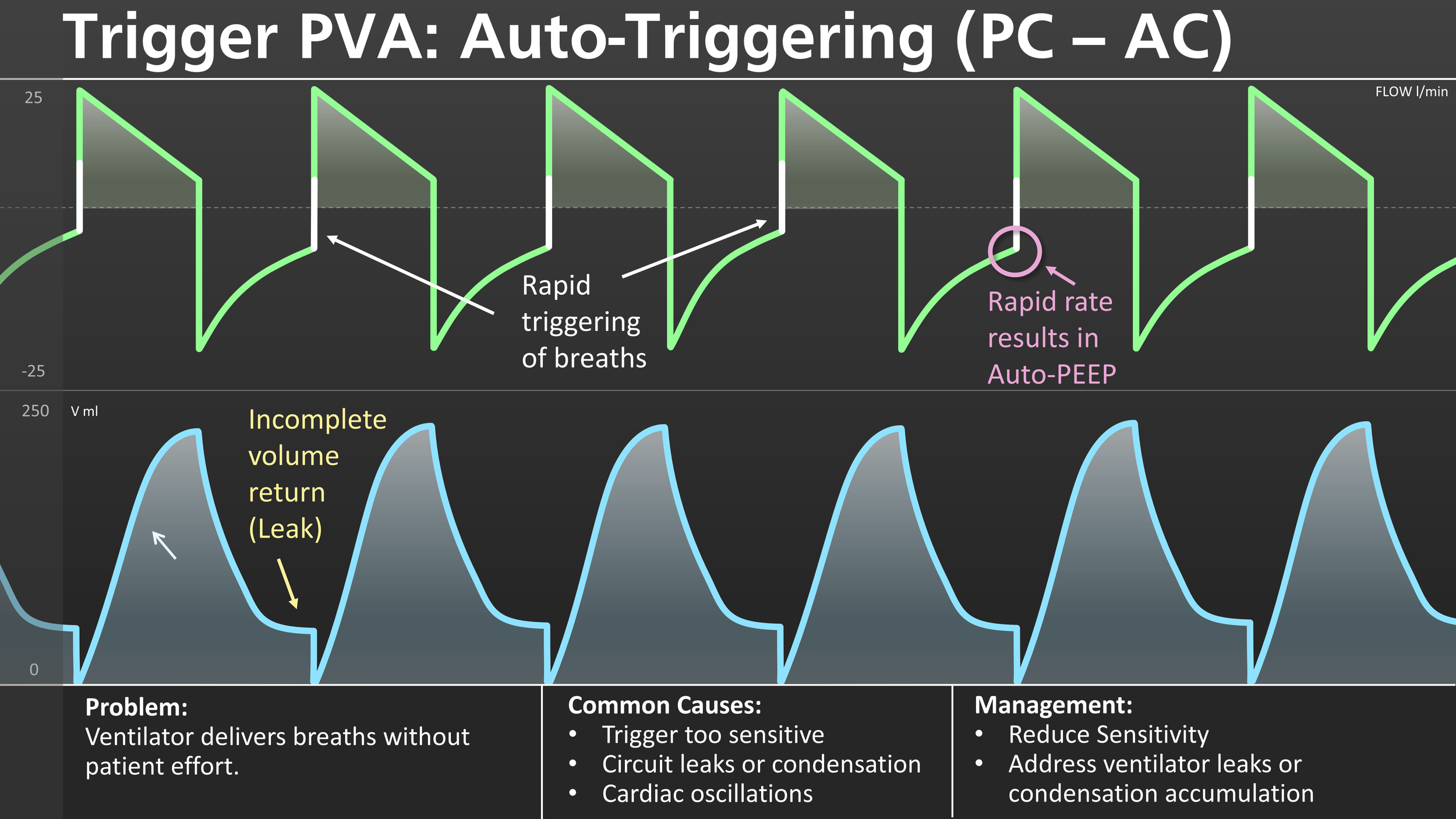
Trigger PVA: Auto-Triggering
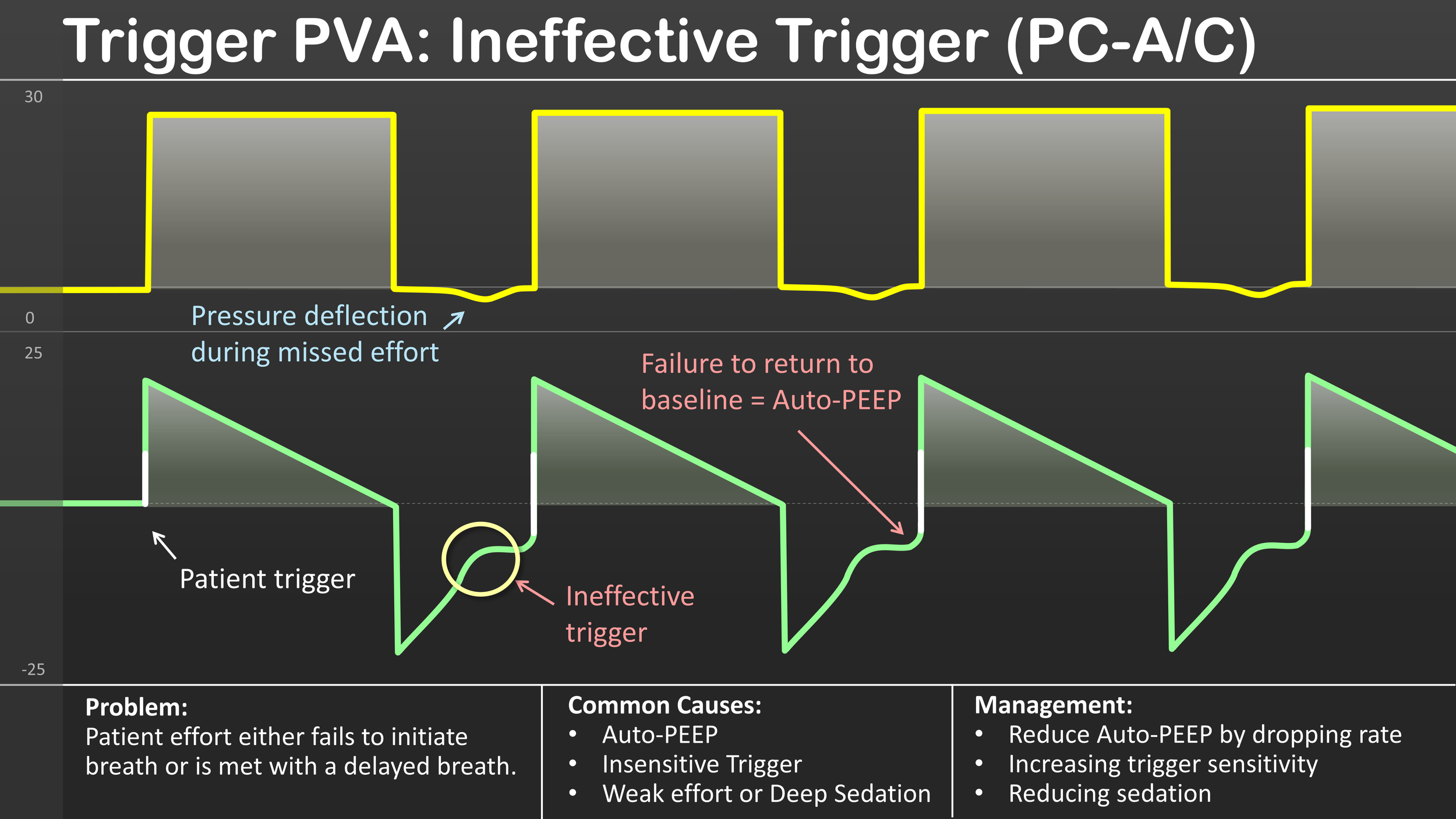
Trigger PVA: Ineffective Trigger
Ineffective triggering is a form of patient-ventilator asynchrony (PVA) that occurs when the patient attempts to initiate a breath but the ventilator fails to recognize the effort. This failed trigger is reflected as a negative deflection on the pressure scalar, and a corresponding positive inflection during the expiratory phase on the flow scalar. This failure of the ventilator to recognize patient effort can be met either with a delayed breath or no breath at all.
Common Causes
Typically, ineffective triggering is caused by the accumulation of Auto-PEEP (air trapping). This occurs when there is residual air that remains in the lungs at the end of exhalation due to inadequate expiratory time. This can cause a situation where the intrinsic pressure must be overcome before a breath can be triggered. Other common factors that may lead to ineffective triggering include:
Weak inspiratory effort (e.g., sedation, fatigue, diaphragm atrophy, etc.)
Insensitive trigger setting.
Why It Matters
As in all forms of PVA, ineffective triggering may cause increased work of breathing which may lead to discomfort, ventilator-induced lung injury (VILI) and can delay liberation from mechanical ventilation.
Management
Decrease auto-PEEP (increase expiratory time, reduce rate or tidal volume)
Increase trigger sensitivity (make it easier to trigger a breath)
Optimize sedation and assess for respiratory muscle weakness
Clinical Pearl: If the patient seems like they are trying to breathe but the ventilator is not responding to their effort, think ineffective trigger and focus on diagnosing the underlying cause.

Systematic ABG Interpretation

Chest X-Ray Interpretation
I recently started assisting a cohort at a local university and made this graphic to help them with their interpretation of X-rays. A million things could be added to this however, you have to start somewhere. Like anything else, it can be helpful to systematize your approach. Hope this helps.

Phase Variable Taxonomy
When talking about different modes of ventilation, it is important to be speaking the same language as everyone else. For this purpose, it can be helpful to use a classification system. The one I find to be the most useful in breaking down how ventilator modes work is phase variable taxonomy. It may sound intimidating, but at it’s most fundamental, it is just breaking down the ventilator modes into 3 phases. The trigger phase (what starts the breath), the limit phase (what constrains or limits inspiration without ending it), and the cycle phase (what ends inspiration and begins exhalation). I’ve broken this down into a one page reference guide, as well as several more focused slides to help solidify this concept. Hope this helps!

APRV-TCAV (One Pager)

Automode (One Pager)
Automode (One Pager)
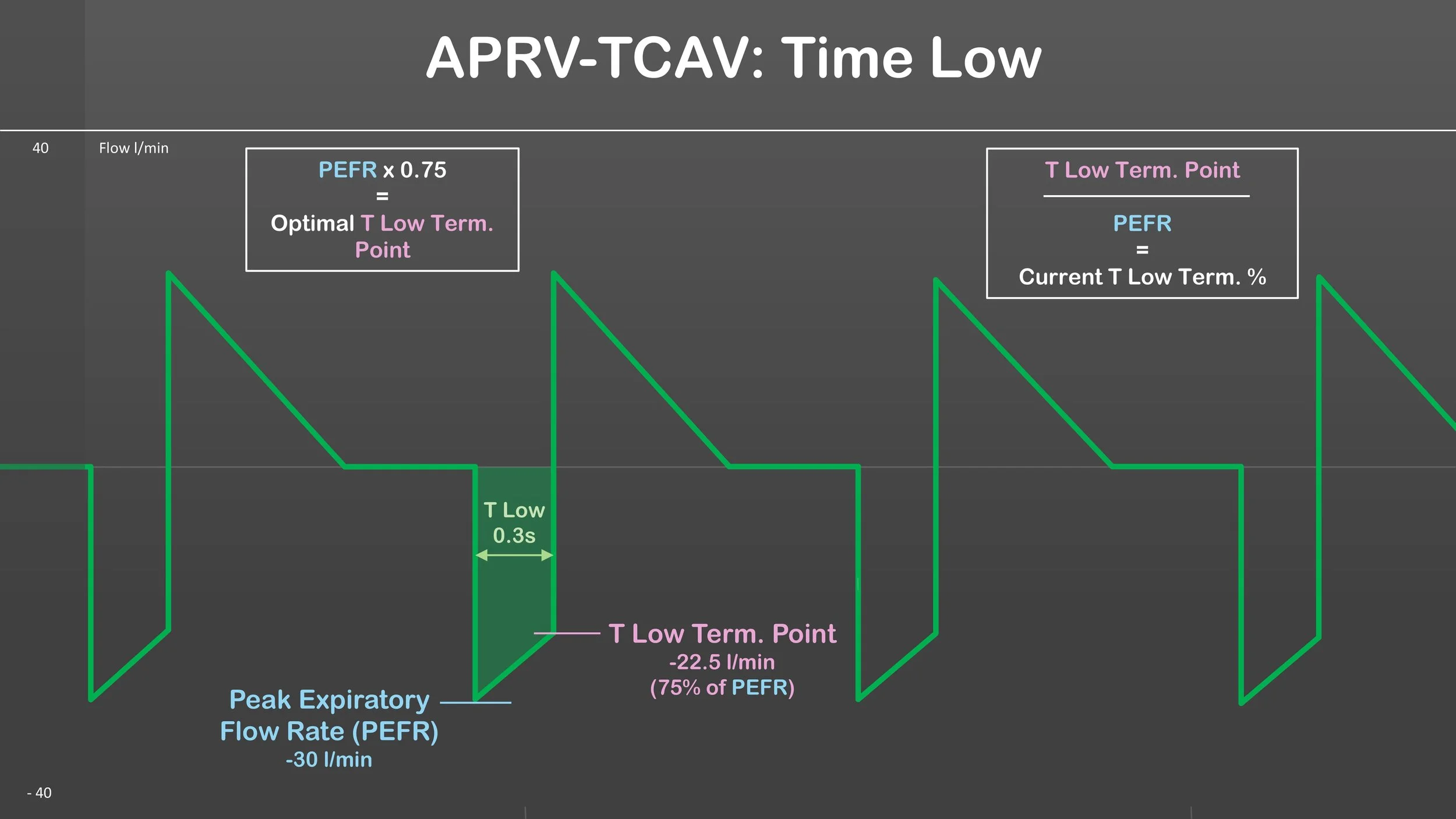
APRV-TCAV: Time Low
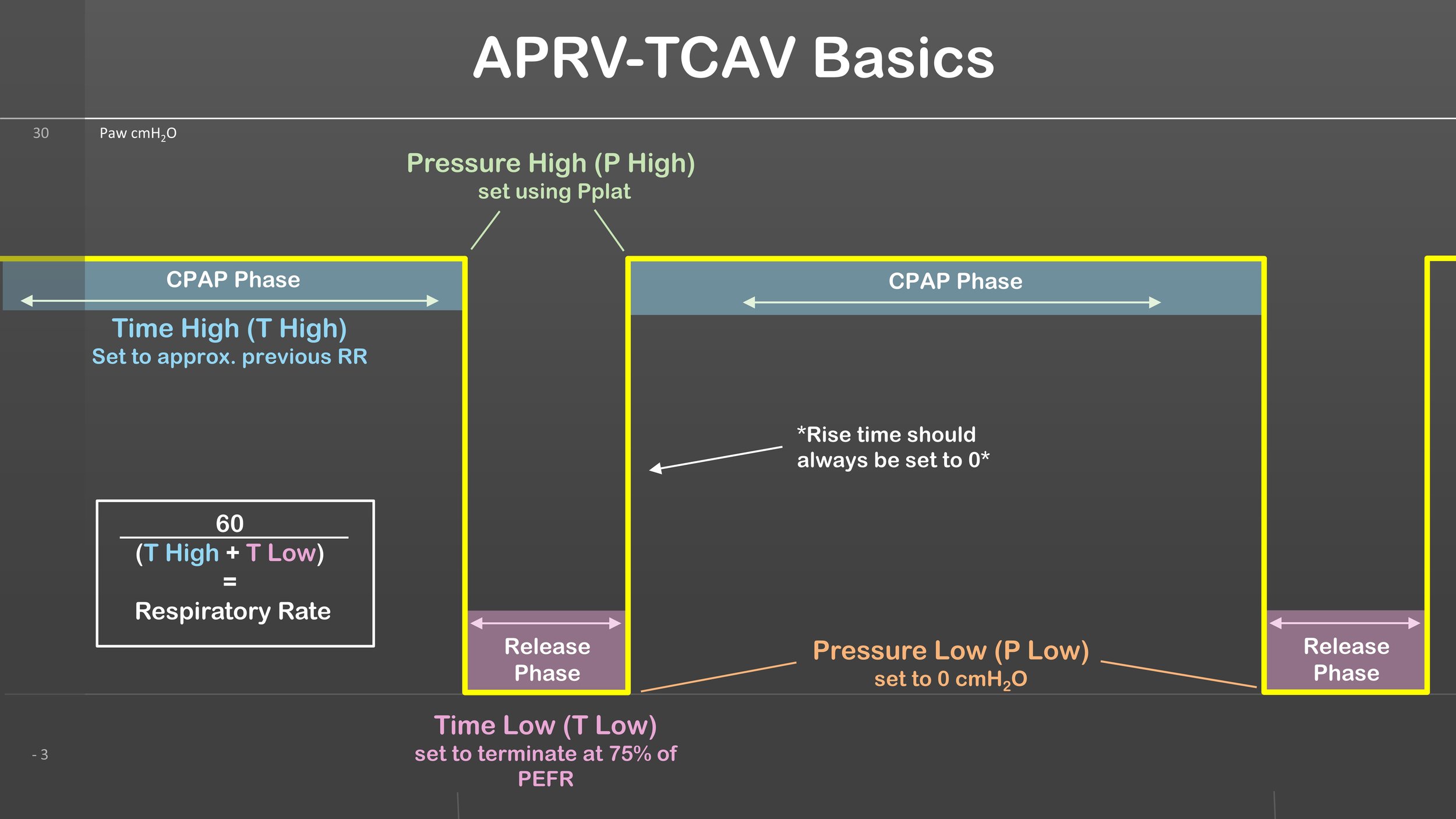
APRV-TCAV Basics

Pulmonary Vascular Resistance Curve
When treating patients sensitive to changes in pulmonary vascular resistance (PVR), such as those with right heart failure or pulmonary hypertension, it's crucial to understand how lung volumes affect PVR.
To clarify, we can categorize the pulmonary vasculature into two types: intra-alveolar and extra-alveolar vessels.
Intra-alveolar vessels are found within alveolar ducts and walls, where gas exchange occurs. As the lungs inflate, the capillaries in the alveolar septal walls become compressed, increasing intra-alveolar PVR.
Extra-alveolar vessels, which are connected to lung parenchyma, distend or elongate during lung inflation. An important factor here is hypoxic vasoconstriction: in regions of atelectasis, the lack of oxygen leads to vessel constriction, causing intra-pulmonary shunting. This reduces gas exchange efficiency and raises PVR.
The overall PVR curve follows a U-shape, with the optimal balance occurring at functional residual capacity (FRC). At this point, intra-alveolar vessels are minimally compressed, and extra-alveolar vessels are adequately distended.
Clinical application: For example, when treating a patient with severe pulmonary hypertension, a chest X-ray revealed hyperinflation (10 ribs expanded) and darkened hilar regions. Recognizing that hyperinflation could place the patient at the high end of the PVR curve, we decreased PEEP, which led to an immediate increase in SpO2 from the low 90s to 100%. This allowed us to gradually reduce nitric oxide and FiO2 as well.
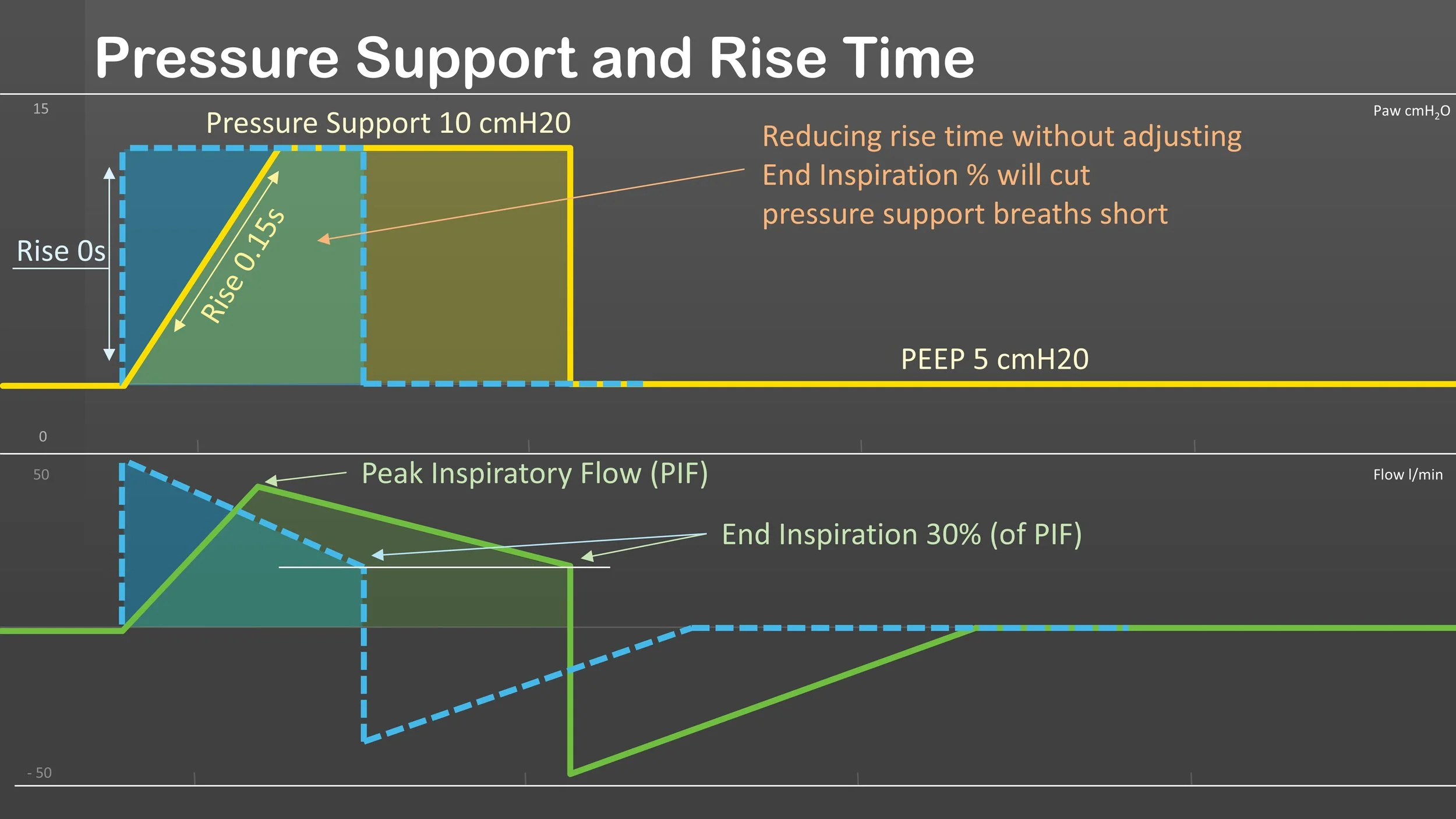
Pressure Support and Rise Time
Rise time is a valuable tool for improving patient synchrony during mechanical ventilation. However, it’s important to remember that on many ventilators, the rise time setting affects both control and pressure support breaths. This becomes especially relevant in modes that combine SIMV and pressure support.

Ventilator Mode Cheat Sheet
In most cases, it is not the mode you choose but how you choose to use it. With that being said, every patient is different, and every mode goes about accomplishing the tasks of ventilation and oxygenation a bit differently. Hope this helps clear up some of the major differences.

“Cycling Down” PRVC
PRVC can become problematic in patients with increased ventilatory demand and respiratory drive (febrile peds, sepsis, DKA, neuro, etc.).

Time Constants
Time Constant = Resistance x Compliance
A time constant is the time it takes for a 63% change in lung volume. Three time constants account for 95% of the volume change. Time constants can be used for inspiration as well as exhalation; however, expiratory time constants tend to be more accurate and useful for determining compliance due to exhalation typically being a passive phase. Increased compliance or resistance leads to longer or shorter time constant values and different lung areas may have varying time constants. This is especially important for patients with obstructive diseases like BPD and COPD.

ABG Interpretation
compensation at the bottom of the graphic. I will be posting a video next week breaking down the process of using this sheet. I hope you all will find this useful.